

A Brief History Of Detransition
For Detrans Awareness Day 2026

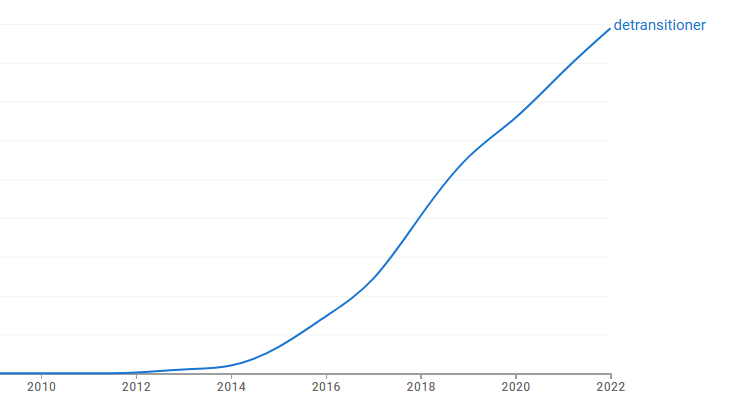
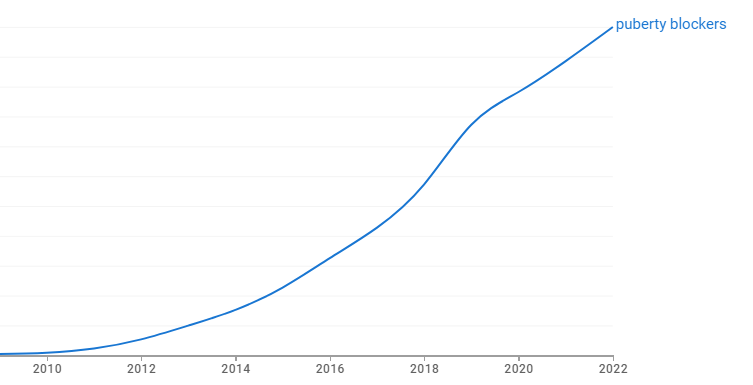
As shown by these two graphs, the rising number of published references to “detransitioner” has closely tracked the rise in published references to “puberty blockers”. The graph looks very different when both terms are compared together because detransitioners get far less attention than ‘trans kids’. We have to see them independently to discern the pattern.
This is mathematical evidence that transgender medicine creates detransitioners. The sudden arrival of transgender medicine and lifestyles for kids after 2011, when Jazz Jennings received his implant, produced the current population of desisting, detransitioning, or ex-trans people. They are not a right-wing plot against the innocent transes. They are the discarded byproduct of transgender ideology.
During 2010, Ångrarna, or “Regretters,” a 2010 film by Marcus Lindeen, presented the world with its first documentary about surgical transition regret. The film won awards, including the Prix Europa for best documentary, receiving praise from the wokeratti for its exploration of the ‘gender journey’ both men had traveled.
Mikael Johansson was an autogynephile. Orlando Fagin was a homosexual transsexual. Like Ritchie Herron, a British detransitioner who has appeared in more recent documentaries, Johansson regretted his surgery instantly upon awakening. Fagin lied about his sex to marry a man, with predictable drama when the truth became impossible to hide anymore.
Both men were convinced that “sex change” was real. Both were still grappling with the complications that surgical transition created in their lives because “sex change” is a lie. Every ex-trans person has a different story, but every story shares this one lie that people believed about themselves, that they no longer believe.
Fagin and Johansson lived in a country with single-payer health insurance, and more importantly, centralized bureaucratic record-keeping. In fact, when they appeared onscreen, Sweden was about to become the place where real transition regret rates first gained medical attention and a proactive response from health authorities.

Published during 2014, a study of “sex reassignment surgery” found historical regret rates of approximately 2 percent in the Swedish cohort who had legally changed their sex markers from 1960–2010. In other words, only people who asked for their sex markers to be restored to their birth sex were counted as “regretting” transition. This leaves out, for example, people who regret transition, but choose to remain in their new identity because they have destroyed their sexual function anyway. Regret is not the same thing as detransition.
More importantly, this small figure is already double the constantly-repeated figure of one percent regret that always appears at the first mention of detransition. In a separate, and more famous, 2011 study, Sweden also found that medical transition is absolutely not ‘life-saving’. If anything, suicidality greatly increases and long-term mental health suffers.
By now, I have interviewed or gotten to know dozens of people who regret their medicalization, and few ever gave the clinicians who harmed them any feedback. Loss to follow-up is notorious at gender clinics. For a variety of reasons, it was always clear that the actual rate of actual regret was never being measured by any study.
Moreover, the literature on detransition so far has consistently found 7-10 or 8-11 years as the range of long-term regret, that is, the end of the euphoria, aka the hormone hangover. For all of these reasons, the detransitioner Ngram curve will continue rising even as transgender identification goes out of style, which seems to be happening.
The future of “detransitioners” as a topic will likely have the same social contagion qualities that transgenderism had in the last decade, namely a gender flip, from a 3 to 1 male to female ratio to the opposite. “Detransitioners” will achieve public awareness the same way and probably exhibit a similar boom in population.
History will also record with some irony, given the amount of policy capture involved in the trans phenomenon, that the detransitioner wave began with parents complaining, and mainstream journalists actually doing their job, followed by action from responsive public health professionals — all in a socialist country.
During 2018, the late Avi Ring started GENID (Gender Identity Project Scandinavia), an association of parents and former patients who worried that children were receiving risky interventions with irreversible effects. For reasons that remain unclear, activists failed to cancel GENID before it got enough attention to the issue that responsible people looked into it.
The following year, the Swedish Public Television program Mission: Investigate produced “The Trans Train and the Teenage Girls” (Tranståget och tonårsflickorna), the first of four episodes focused on the issue. As the series ended in 2023, Sweden was pulling the plug on puberty blocker experiments.
Dr. Sven Roman, a Swedish child and adolescent psychologist, says that no one should undergo medical transition until the age of 25. Psychosocial treatment — therapy aimed at helping kids to cope with adolescence — should be the first treatment for gender dysphoria in youth. Roman submitted a brief to the United States Supreme Court in the Skrmetti case that upheld state bans on pediatric transition ‘medicine’.
The identity of the first person to detransition has yet to be established. Isolated cases appear in medical literature from the 1950s, though they are rarely publicized. Earlier publicized or semi-public examples of clinicians acknowledging rare regret do exist, but no one has definitively been singled out as the first person in the world to detransition. This is hardly surprising. Why would such a person volunteer to be first?
The universal experience of the detransitioner is total rejection by the former community that ‘affirmed’ them. They lose all their friends, and they have almost always hurt their families. If every parent affected by the transgender craze was able to file a million-dollar lawsuit today, the pediatric clinics would all shutter tomorrow. The path back is emotionally and psychically fraught. Some do not make it.
Surgical transition is irreversible, but chemical transition also has irreversible effects. Nonmedical interventions are not harmless, either: binders can harm ribcages and tucking can harm testicles. Even social transition has severe mental health impacts. The a la carte nature of gender medicine, with its focus on ‘embodiment goals’, produces this descending order of harms.
As a result, the detransitioned population requires complex care, such as a differentiation of therapy groups — social desisters in one, chemical and surgical detransitioners in others. Anyone who leaves transition behind now will find resources and organizations, such as Genspect, that did not exist just a few years ago because demand has already grown so much in so little time.
I will be in Washington, DC tomorrow to report from Detrans Awareness Day 2026. Last year brought all sorts of good policy news on this front. Studies of insurance claims have found that tens of thousands of children had various interventions, thousands of them surgical ones. Recently, the first detransitioned litigant won $2 million from a blue New York jury. While detransition is a new historical phenomenon, it has quite a future.